What is the historical understanding of CBR?
The definition for community-based rehabilitation has undergone many changes, beginning with its inception in the 1980s.
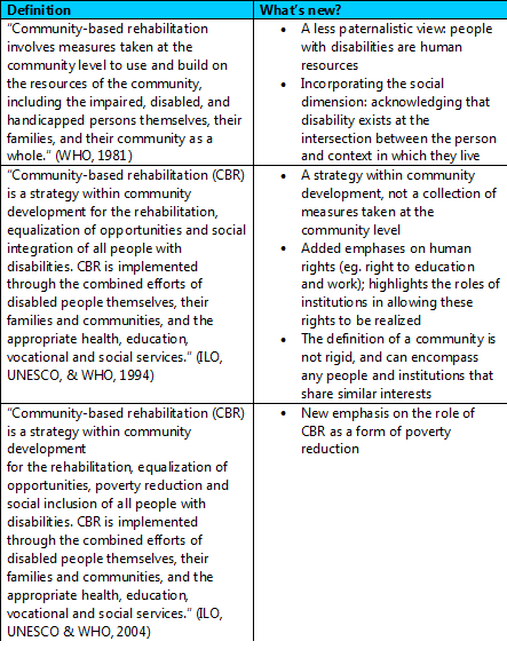
What is the current understanding of CBR?
CBR is a primary health care initiative and comprehensive social model for addressing rehabilitation care in a community setting. It emphasizes community participation, empowering the community to direct their own rehabilitation care, reinforcing human rights of persons with disabilities, and using existing community resources (Sharma, 2004). Importantly, it extends the biomedical model of disability to incorporate social concerns, such as the exclusion of persons with disabilities from mainstream education and discrimination in health services. Its development has been driven by participation from stakeholders in disability activism and persons with disabilities (Hartley, Finkenflügel, Kuipers, & Thomas, 2009).
CBR has been applied in more than 80 countries through top-down and bottom-up initiatives. It has been used in conjunction with hospital services, offered as a component of structural development programs by non-governmental organizations, and directed by communities without external assistance (Sharma, 2004; Pollard & Sakellariou, 2008).
CBR has been applied in more than 80 countries through top-down and bottom-up initiatives. It has been used in conjunction with hospital services, offered as a component of structural development programs by non-governmental organizations, and directed by communities without external assistance (Sharma, 2004; Pollard & Sakellariou, 2008).
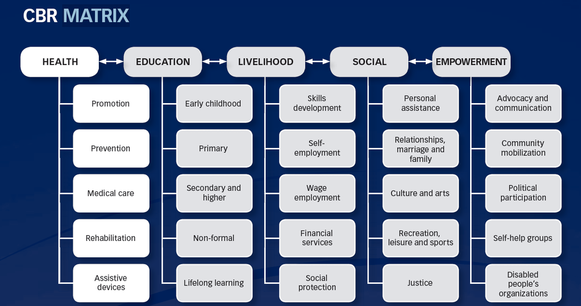
The WHO and its partner organizations have played a pivotal role in promoting the most recent definition of CBR, and also in creating a comprehensive set of CBR guidelines. The new understanding of CBR can be represented by the CBR matrix which includes 5 major dimensions of rehabilitation: health, education, livelihood, social, and empowerment (ILO, UNESCO & WHO, 2010).
CBR emphasizes the use of mainstream, existing resources, such as health facilities, educational institutions, community services, and non-governmental organizations (ILO, UNESCO & WHO, 2010). The wider referral network can be illustrated by a circle radiating outward, beginning with the individual with disability and their immediate support network, and ending with the national "community".
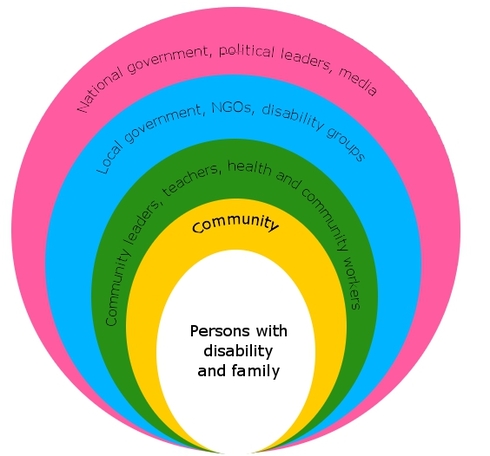
(ILO, UNESCO & WHO, 2010)
For a detailed guide to running a CBR program, click here.
What are the common characteristics of CBR programs?
Although CBR programs vary, common elements of sustainable programs include:
For examples of CBR programs that already exist, click here.
- National level support in coordinating resources and policies
- A human rights-based approach
- Voluntary participation from the community
- Motivated community health workers
For examples of CBR programs that already exist, click here.
Intended outcomes of CBR:
- Individual and community knowledge of disabilities increases
- The community is involved in their own rehabilitation care, and rehabilitation is delivered with collaboration from various sectors of society
- Discrimination on the basis of disability and other factors (eg. gender) in the health sector is reduced
- Access to rehabilitation services is improved
- Persons with disabilities more actively participate in education, work, and community life
References:
Finkenflügel, H., Wolffers, I., & Huijsman, R. (2005). The evidence base for community-based rehabilitation: A literature review. International Journal of Rehabilitation Research, 28(3), 187-201.
ILO, UNESCO & WHO. (1994). Community-Based Rehabilitation for and with People with Disabilities: Joint Position Paper. Geneva: United Nations.
ILO, UNESCO & WHO (2004). Community-based rehabilitation for and with people with disabilities. Joint Position Paper. Geneva: United Nations.
ILO, UNESCO & WHO (2010). Introductory booklet - Community-based rehabilitation - CBR guidelines. Geneva: United Nations.
Pollard, N., & Sakellariou, D. (2008). Operationalizing community participation in community-based rehabilitation: Exploring the factors. Disability and Rehabilitation, 30(1), 62-70.
Sharma, M. (2004). Viable methods for evaluation of community-based rehabilitation programs. Disability and Rehabilitation, 26(6), 326-334.
WHO. (1981). Disability prevention and rehabilitation. Geneva, Switzerland: WHO.
Finkenflügel, H., Wolffers, I., & Huijsman, R. (2005). The evidence base for community-based rehabilitation: A literature review. International Journal of Rehabilitation Research, 28(3), 187-201.
ILO, UNESCO & WHO. (1994). Community-Based Rehabilitation for and with People with Disabilities: Joint Position Paper. Geneva: United Nations.
ILO, UNESCO & WHO (2004). Community-based rehabilitation for and with people with disabilities. Joint Position Paper. Geneva: United Nations.
ILO, UNESCO & WHO (2010). Introductory booklet - Community-based rehabilitation - CBR guidelines. Geneva: United Nations.
Pollard, N., & Sakellariou, D. (2008). Operationalizing community participation in community-based rehabilitation: Exploring the factors. Disability and Rehabilitation, 30(1), 62-70.
Sharma, M. (2004). Viable methods for evaluation of community-based rehabilitation programs. Disability and Rehabilitation, 26(6), 326-334.
WHO. (1981). Disability prevention and rehabilitation. Geneva, Switzerland: WHO.
